 E-submission
E-submission
Search
- Page Path
- HOME > Search
Original Article
- The diagnostic value of circulating tumor DNA in hepatitis B virus induced hepatocellular carcinoma: a systematic review and meta-analysis
- Young Chang, Soung Won Jeong, Jae Young Jang, Hyuksoo Eun, Young‑Sun Lee, Do Seon Song, Su Jong Yu, Sae Hwan Lee, Won Kim, Hyun Woong Lee, Sang Gyune Kim, Seongho Ryu, Suyeon Park
- J Liver Cancer. 2022;22(2):167-177. Published online September 29, 2022
- DOI: https://doi.org/10.17998/jlc.2022.09.19
- 2,583 Views
- 72 Downloads
- 1 Citation
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material - Background/Aim
New biomarkers are urgently needed to aid in the diagnosis of early stage hepatocellular carcinoma (HCC). We performed a meta-analysis on the diagnostic utility of circulating tumor DNA (ctDNA) levels in patients with hepatitis B virus-induced HCC.
Methods
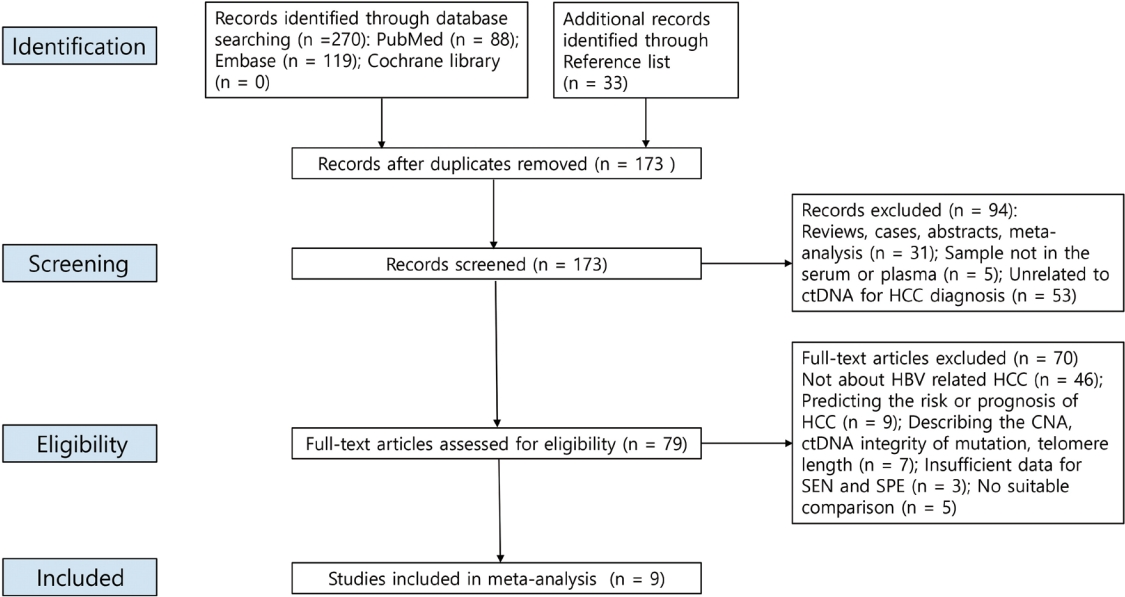
We retrieved relevant articles from PubMed, Embase, and the Cochrane Library up to February 8, 2022. Two subgroups were defined; one subset of studies analyzed the ctDNA methylation status, and the other subset combined tumor markers and ctDNA assays. Pooled sensitivity (SEN), specificity (SPE), positive likelihood ratio (PLR), negative likelihood ratio (NLR), diagnostic odds ratio (DOR), and area under the summary receiver operating characteristic curve (AUC) were analyzed.
Results
Nine articles including 2,161 participants were included. The overall SEN and SPE were 0.705 (95% confidence interval [CI], 0.629-0.771) and 0.833 (95% CI, 0.769-0.882), respectively. The DOR, PLR, and NLR were 11.759 (95% CI, 7.982-17.322), 4.285 (95% CI, 3.098- 5.925), and 0.336 (0.301-0.366), respectively. The ctDNA assay subset exhibited an AUC of 0.835. The AUC of the combined tumor marker and ctDNA assay was 0.848, with an SEN of 0.761 (95% CI, 0.659-0.839) and an SPE of 0.828 (95% CI, 0.692-0.911).
Conclusions
Circulating tumor DNA has promising diagnostic potential for HCC. It can serve as an auxiliary tool for HCC screening and detection, especially when combined with tumor markers. -
Citations
Citations to this article as recorded by
- 16S rRNA Next-Generation Sequencing May Not Be Useful for Examining Suspected Cases of Spontaneous Bacterial Peritonitis
Chan Jin Yang, Ju Sun Song, Jeong-Ju Yoo, Keun Woo Park, Jina Yun, Sang Gyune Kim, Young Seok Kim
Medicina.2024; 60(2): 289. CrossRef
- 16S rRNA Next-Generation Sequencing May Not Be Useful for Examining Suspected Cases of Spontaneous Bacterial Peritonitis

Case Reports
- Long-term survival after CCRT and HAIC followed by ALPPS for hepatocellular carcinoma with portal vein invasion: a case report
- In-Jung Kim, Sung Hwan Yoo, Jung Il Lee, Kwan Sik Lee, Hyun Woong Lee, Jin Hong Lim
- J Liver Cancer. 2022;22(1):84-90. Published online March 22, 2022
- DOI: https://doi.org/10.17998/jlc.2022.03.07
- 2,790 Views
- 70 Downloads
- 1 Citation
-
Abstract
PDF
- There are various methods for treating advanced hepatocellular carcinoma with portal vein invasion, such as systemic chemotherapy, transarterial chemoembolization, transarterial radioembolization, and concurrent chemoradiotherapy. These methods have similar clinical efficacy but are designed with a palliative aim. Herein, we report a case that experienced complete remission through “associating liver partition and portal vein ligation for staged hepatectomy (ALPPS)” after concurrent chemoradiotherapy and hepatic artery infusion chemotherapy. In this patient, concurrent chemoradiotherapy and hepatic artery infusion chemotherapy induced substantial tumor shrinkage, and hypertrophy of the nontumor liver was sufficiently induced by portal vein ligation (stage 1 surgery) followed by curative resection (stage 2 surgery). Using this approach, long-term survival with no evidence of recurrence was achieved at 16 months. Therefore, the optimal use of ALPPS requires sufficient consideration in cases of significant hepatocellular carcinoma shrinkage for curative purposes.
-
Citations
Citations to this article as recorded by- Is multidisciplinary treatment effective for hepatocellular carcinoma with portal vein tumor thrombus?
Won Hyeok Choe
Journal of Liver Cancer.2022; 22(1): 1. CrossRef
- Is multidisciplinary treatment effective for hepatocellular carcinoma with portal vein tumor thrombus?
- A Case of Focal Nodular Hyperplasia-like Nodules in Cirrhosis
- Young Joon Yoon, Ki Tae Yoon, Jun Yong Park, Hyun Woong Lee, Hwa Sook Kim, Jae Kyung Kim, Young Nyun Park, Kwang-Hyub Han, Chae Yoon Chon, Young Myung Moon, Mi-Suk Park, Sang Hoon Ahn
- Journal of the Korean Liver Cancer Study Group. 2007;7(1):41-44. Published online June 30, 2007
- 719 Views
- 37 Downloads
-
Abstract
PDF
- Focal nodular hyperplasia (FNH) usually occurs in non-cirrhotic livers and was defined as a nodule composed of benign appearing hepatocytes occurring in a liver that is otherwise histologically normal or nearly normal. However, due to improvements in imaging techniques and pathological evaluation of explant livers, a focal lesion that is very similar to the classic form of focal nodular hyperplasia that occurs in cirrhotic liver has been described by several reports. Therefore, the term FNH-like nodules has been proposed. In this report, we report a case of focal nodular hyperplasia-like nodules in cirrhosis. A 59 year old woman with known hepatitis B virus infection visited our institution for routine check up. She was diagnosed as having liver cirrhosis and 3.5 cm sized liver mass on abdomen ultrasonography (US). Because tumor marker was negative and US findings are not compatible with hepatocellular carcinoma, other imaging modalities were performed. Magnetic resonance imaging (MRI) documented a 3.5 cm sized hypervascular nodule with internal aberrant vascular structure and multiple small sized nodules in remaining liver. Needle biopsy was targeted to the liver main mass. Microscopic finding revealed FNH-like nodule and underlying liver cirrhosis.
- Excellent Response to Hepatic Arterial Infusional Chemotherapy in Advanced Hepatocellular Carcinoma with Portal Vein Thrombosis
- Keun-Ho Lee, Ja Kyung Kim, Kwang-Hyub Han, Jong Tae Lee, Do Youn Lee, Jong Yoon Won, Hyun Woong Lee, Hwa Sook Kim, Ki Tae Yoon, Sang Hoon Ahn, Chae Yoon Chon, Young Myoung Moon
- Journal of the Korean Liver Cancer Study Group. 2006;6(1):42-46. Published online June 30, 2006
- 524 Views
- 0 Download
-
Abstract
PDF
- There is no treatment of curative aim in advanced hepatocellular carcinoma (HCC) with portal vein thrombosis (PVT), which is associated with poor prognosis. Albeit one of the treatment options is intra-arterial infusional chemotherapy, its therapeutic efficacy was minimal. In this report, we present an unusual case of a patient with favorable result after intra-arterial infusional chemotherapy. This patient was HBV carrier and diagnosed having HCC of stage IVb (T4N0M1) with right PVT on February 1999. Direct right adrenal gland and right kidney invasion and numerous intrahepatic metastases were also noted. The serum AFP level showed more than 60,000 ng/mL, and the Child-Pugh score was 5 (class A). The patient received three sessions of intra-arterial 5-fluorouracil (5-FU) and cisplatin combination chemotherapy and two additional sessions of systemic (5-FU) chemotherapy combined with intra-arterial cisplatin infusion. After total 5 sessions of combination chemotherapy, follow-up CT scan revealed grossly total necrosis of main HCC and numerous intrahepatic metastases, without evidence of viable portion in July 1999. The AFP level decreased to 79.4 ng/mL. The latest CT scan taken in November 2005 also showed no evidence of recurrence. It is noteworthy that the patient with advanced HCC with PVT showed complete remission only after 5 sessions of intra-arterial chemotherapy and the status of complete remission is maintained for more than 76 months.
 First
First Prev
Prev


 Follow JLC on Twitter
Follow JLC on Twitter